Organogenesis
The Gonads - Indifferent Stage
In the first stage of gonadal development, it is impossible to distinguish between the male and female gonad.
The gonads begin as genital ridges – a pair of longitudinal ridges derived from intermediate mesoderm and overlying epithelium. They initially do not contain any germ cells.
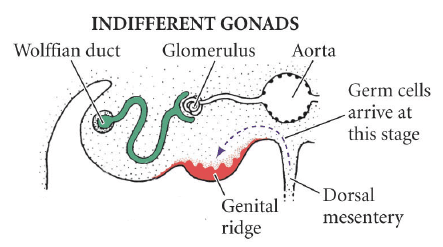
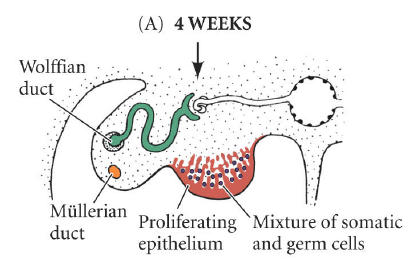
In the fourth week, germ cells begin to migrate from the endoderm lining of the yolk sac to the genital ridges, via the dorsal mesentery of the hindgut. They reach the genital ridges in the sixth week.
Simultaneously, the epithelium of the genital ridges proliferates and penetrates the intermediate mesoderm to form the primitive sex cords.
The combination of germ cells and primitive sex cords forms the indifferent gonad – from which development into the testes or ovaries can occur.
Female gametes (oocytes) all have a 22X chromosomal makeup.
Male gametes (spermatozoa) are either 22X or 22Y.
The chromosomal sex of the fetus is determined at fertilization when the male and female gametes combine; XX is female and XY is male.
A single gene (SRY), located in the sex-determining region of the Y chromosome directs the undifferentiated gonad to become a testis rather than an ovary.
. If the SRY gene is present on the Y chromosome produces testis-determining factor that is required forformation of testes.
In the absence of the SRY gene, gonads will differentiate into ovaries
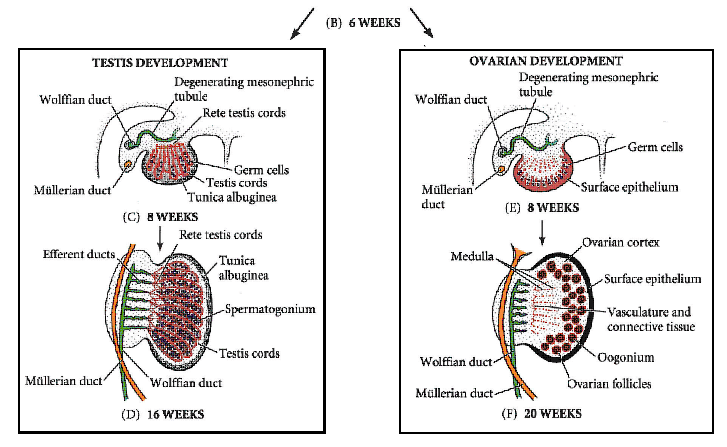
Testes Development << >> Ovarian Development
-
Before sexual differentiation, the fetus has two parallel duct systems located near the undifferentiated gonads: the mesonephric (Wolffian) duct and the paramesonephric (Müllerian) duct.
-
By week 10 of gestation, the fetal gonads can be distinguished as either testes or ovaries.
-
In males, the primordial germ cells give rise to precursors of male gametes called spermatogonia.
-
The germinal epithelium that will later produce male gametes is formed by spermatogonia plus support cells called Sertoli cells.
-
The surrounding mesenchyme becomes Leydig cells, which secrete testosterone.
-
-
In females, the primordial germ cells give rise to precursors of female gametes called oogonia.
-
The epithelium surrounding the oogonia differentiates into granulosa cells, and the surrounding ovarian mesenchyme becomes thecal cells.
-
In the sexually mature female, estrogens and progestins are secreted by the granulosa and theca cells.
-
-
- Differentiation of the genitalia depends only on the presence or absence of hormones secreted by the testes.
-
In the male fetus, the secretion of testosterone by Leydig cells directs each mesonephric duct to develop into an epididymis, a vas deferens, and a seminal vesicle.
-
Leydig cells produce testosterone in response to the hormone human chorionic gonadotropin (hCG), which is secreted by the placenta.
-
The developing Sertoli cells are directed by SRY to secrete Müllerian-inhibiting substance, causing regression of the Müllerian duct system.
-
The absence of the Müllerian-inhibiting substance in the female fetus allows the Müllerian duct system (instead of the Wolffian duct) to develop, leading to formation of the fallopian tubes, the uterus, and the upper vagina.
-
Fetal ovaries are not necessary for the development of the female genitalia due to the high concentration of maternal estrogens that are present during pregnancy.
-
-
Undifferentiated external genitalia consist of a genital tubercle and a urogenital slit, bounded by two lateral genital folds and two labioscrotal swellings.
-
In males, the conversion of testosterone to dihydrotestosterone, via the enzyme 5α-reductase within these target tissues, is necessary for formation of the prostate gland and the male external genitalia.
-
The genital folds fuse to form the penis; the enlargement and fusion of the labioscrotal swellings form the scrotum.
-
Descent of the fetal testes into the scrotum requires the secretion of the fetal gonadotropins and occurs during the last trimester of pregnancy.
-
 Cryptorchidism is the incomplete descent of the testis from the abdominal cavity to the scrotum and is associated with testicular malignancy and infertility. In the setting of unilateral cryptorchidism, the fully descended testis may remain at risk of impaired sperm production or of becoming malignant.
Cryptorchidism is the incomplete descent of the testis from the abdominal cavity to the scrotum and is associated with testicular malignancy and infertility. In the setting of unilateral cryptorchidism, the fully descended testis may remain at risk of impaired sperm production or of becoming malignant.
-
-
In females, the urogenital slit remains open to form the introitus (vaginal opening).
-
The labia minora are formed from the genital folds, and the clitoris forms anterior to the urethral opening.
-
The labia majora are formed from the labioscrotal swellings. Exposure of the female fetus to androgens at this critical time of sexual differentiation can result in masculinization of the fetus, irrespective of the genetic or gonadal sex.
-
Virilization of a fetus refers to a genetic female with normal ovaries and Müllerian duct structures (e.g., fallopian tubes, uterus, and upper vagina), but with masculinization of the external genitalia (e.g., clitoromegaly, fusion of the labioscrotal folds) due to excessive in utero exposure to androgens.
-
-
-
Differences in sexual development (DSD).
-
There are several conditions in which gonadal and phenotypic sex differ.
-
Complete androgen insensitivity syndrome (CAIS) results from the lack of functional androgen receptors and illustrates the role of steroids in sexual differentiation, as follows:
-
CAIS patients are 46 XY DSD. The gonads become testes since the Y chromosome is present; the testes remain undescended.
-
Müllerian-inhibiting substance continues to be secreted from the Sertoli cells, resulting in the absence of the female internal genitalia. Patients have a short, blind-ended vagina without a cervix, uterus, or ovaries.
-
Dihydrotestosterone is made but cannot direct the Wolffian duct to develop into male genitalia due to lack of androgen receptors; individuals have female external genitalia.
-
Masculinization does not occur during puberty because of the lack of testosterone action. Conversion of testosterone to estrogen causes breast development at puberty instead, but there is only a small amount of pubic hair. Diagnosis is often determined following failure of the onset of the menstrual cycle.
-
-
Deficiency of 5α-reductase is another example of 46 XY DSD and causes ambiguous genitalia because it interferes with the conversion of testosterone to dihydrotestosterone.
-
Testosterone is present but is a weaker androgen than DHT leading to varying degrees of failure of the genital and labioscrotal folds to close.
-
Masculinization at puberty can occur because androgen receptors are present and respond to testosterone, distinguishing this condition from CAIS.
-
-
Congenital adrenal hyperplasia (CAH) is the most common reason for ambiguous genitalia in 46 XX DSD individuals.
-
Deficiency of the enzyme 21-hydroxylase in the steroid synthesis pathway is the most common cause of CAH and results in excessive production of adrenal androgens and virilization of a female fetus.
-
-
Puberty
Anatomic differentiation into male or female occurs in utero, but the final maturation of fully functional reproductive organs is not completed until puberty.